
This article is intended to provide insight into the differences between an acute vs chronic ankle sprain. Please refer to our article regarding acute lateral ankle sprains for more information about a recently-occurring and first-time lateral ankle sprain
*** When we use the term “chronic”, we are referring to long-standing pain or dysfunction that never fully resolved, as opposed to more complex nervous system conditions such as central sensitization or complex regional pain syndrome.
What is a chronic ankle sprain?
A chronic ankle sprain refers to a history of ankle sprains that never fully resolved, or an ankle that is constantly sprained, usually due to chronic ankle instability.
How do you end up with a chronic ankle sprain?
Usually, but not always, a chronic ankle sprain begins with an acute event, such as a moderate to severe lateral ankle sprain, other low ankle sprain, or a high ankle sprain, that occurs as a result of aggressively rolling the ankle.
If not properly treated, especially in the sense of improving strength and stability, one can develop chronic ankle instability, meaning you will be more vulnerable to future ankle sprains.
As a general rule, the higher number of ankle sprains, the higher the risk of developing chronic ankle instability, especially if not treated properly through strength and stability exercises.
Those with more systemic conditions that cause excessive movement in the joints, such as Ehlers-Danlos Syndrome, will also be at higher risk of frequent ankle sprains due to chronic ankle instability. In this case, strength and stability exercises become increasingly important, not just for prevention of ankle sprains, but for all injuries to all joints in the body that are exposed to large forces.

Why does can an ankle sprain lead to chronic ankle instability?
The term “sprain” refers to the stretching and subsequent injury of ligaments. Therefore, with ankle sprains, you are actually damaging, sometimes even tearing, one or more ligaments that cross the ankle.
It’s also important to recognize that ligaments are passive tissues, meaning they cannot be actively and/or voluntarily controlled.
You can think of ligaments as thick and strong elastic bands that help secure a joint. They have some ability to stretch and accommodate motion, but their role is to provide stability to a joint, so they should be somewhat tight.
Given that ligaments are passive structures, they are at the mercy of forces placed on them. When they become stretched to the point of damage, it can be difficult for them to heal to their original length. If they are repeatedly stretched and injured, this can lead to chronic ankle instability.

If not protected properly in the early stages of recovery, the ligaments may heal in a longer position, meaning they don’t provide the same level of stability to the ankle joint, and the joint becomes looser.
If a ligament that crosses the ankle joint is fully ruptured and you keep injuring the ankle, this may lead to even more significant chronic ankle instability.
In order to prevent chronic ankle instability, it’s very important to focus on ankle strength and stability while rehabbing the ankle sprain. Many people stop their rehab when their pain goes away, but reducing pain is just one component of rehab, and to prevent future ankle sprains, it is imperative to return an ample level of support to the ankle joint, which is basically the case for properly rehabbing any ankle injury.
Assessing a Chronic Ankle Sprain
In the case of acute ankle sprains, much of the focus during the assessment will be on the ankle itself with and the specific mechanism of injury, immediate response of the ankle, and the necessity to differentiate an ankle sprain vs. fracture. In this case, patients are often walking with a limp or even non-weight bearing altogether.
Furthermore, there is likely to be some visible bruising and swelling on the lateral aspect of the ankle down to the foot. The area is likely to be visibly inflamed and extremely tender on palpation. In these very acute phases, the ankle is highly sensitive and much of the testing may be provocative, even if not directly stressing the injured ligament.
For a chronic ankle sprain, patients will often describe a history of multiple sprains or “tweaks” that may vary in terms of mechanism of injury.
When listening to the patient’s history of lower body injury, it’s prudent to gain an understanding of their injury history and any other medical conditions that could be influencing the patient’s presentation. It’s not uncommon that I hear something along the lines of, “I basically have a chronic ankle sprain, so I feel like I always have an ankle injury on this side and that it’s always the one getting hurt.”
In this sense, the subjective history may be a little more vague, whereas their description of how it is currently interfering with their lives can be quite specific. Objectively, patients often present with mild swelling around the lateral or medial malleolus, sometimes bruising if they recently aggravated it (“acute on chronic”), and pain when directly testing compromised ligaments, joints, and tendons.
Their symptoms appear to be more localized, and while their ankle may look fairly normal at first glance, functional testing will typically reveal major side-to-side differences. Typically, those with chronic lateral ankle pain will report feeling less stable, or at the very least, this will be picked up during the physical testing.
I have also seen patients in the clinic who have been dealing with chronic ankle pain for a very long time. Typically, these folks are managing their injury/pain reasonably well; however, they are often motivated to seek care when it finally interferes with performing an activity they love to do.
While much of this condition can be treated similarly to an acute lateral ankle sprain, there will likely be some differences to the treatment approach for acute vs. chronic ankle sprains.
Strength Testing for a Chronic Ankle Sprain
When performing manual muscle testing, it’s fairly common to identify weakness with or without pain in the peroneal muscle group, also known as the fibular muscle group. This group consists of peroneus longus, peroneus brevis, and peroneus tertius, and these muscles are highly important in protecting against a lateral ankle sprain.
The peroneal tendons wrap underneath the lateral malleolus to insert on various points of the foot, including the fifth metatarsal and bottom of the foot. These muscles are highly responsible for eversion of the ankle, which is the opposite of inversion, the latter of which happens when you roll your ankle.

Consider these muscles as the first line of defence against an inversion sprain. If they are not strong or responding quickly enough to external forces, they may fail, ultimately placing the burden of the external load on the passive ligamentous structures, such as the ATFL. In chronic cases, it is common to see weakness and/or pain when testing the strength of these muscles in isolation.
Ligament Testing for a Chronic Ankle Sprain
Ligament testing is performed much in the same way as we would with an acute ankle sprain; however, if the ankle is much less irritable than an acute injury, the testing may be a little more comprehensive and the clinician may be able to pick up on more subtle differences in laxity.
Generally speaking, it is quite common to pick up some laxity in the lateral ankle ligaments, namely the ATFL and CFL. However, laxity and/or damage may be more widespread as well depending on the number and severity of previous injuries, and how the patient has adapted their mechanics to compensate for the reduced function of these ligaments.
People are often surprised when they are told a ligament appears to have been fully ruptured at some point, especially when the testing is largely pain-free. This suggests that the injury occurred some time ago, whereas more pain with the testing can suggest a partial tear, or more recent tear.
Even though this is still in the assessment phase, it’s typically an effective time to begin educating the patient about the importance of improving strength around the ankle for the sake of improve stability.
Functional Testing for a Chronic Ankle Sprain
Functional testing for chronic ankle sprains is very similar to the testing we would perform during more advanced phases of recovery from an acute ankle sprain. The reason we can often perform these tests earlier with chronic sprains is because of relatively minimal irritability.
Functional testing often starts with a progression of tests, and while this will vary depending on how the patient in front of me is presenting, I will provide a more general example of stability testing progressions below:
1. Static single leg balance eyes open
2. Static single leg balance eyes closed
3. Static single leg balance eyes open on an unstable surface (e.g. blue foam pad, stack of towels, bosu ball, wobble board, etc)
4. Static single leg balance eyes closed on an unstable surfaces
5. Single leg squat firm surface eyes open
6. Single leg squat unstable surface eyes open
7. Single leg weight acceptance on stable, then unstable surface (e.g. lunge onto bosu)
It’s not always necessary to progress thorough advanced stability testing in the initial assessment, as it can become quickly apparent if there is a side-to-side difference in single leg stability.
Patients are often shocked, sometimes feeling a little embarrassed, at how one side performs relative to the other, so it’s worth mentioning to them that this simply allows us to focus on the relevant impairments and optimize their ankle rehab program.

How do you treat a chronic ankle sprain?
Treatment for a chronic ankle sprain will have a significant emphasis on improving ankle strength, stability, and proprioception.
Assuming an acute injury is ruled out, particularly fractures, muscle strains, and ligament sprains, then it’s typically advised to begin strengthening as guided through physical therapy. Different physical therapists may have different specific strategies, so I will keep it general with my overall strategy as the focus.
Even if the patient is presenting quite well and can perform various stability exercises on their feet, it is often recommended to include at least one resistance band exercise target specific muscle groups, namely the peroneals, especially if a significant weakness is picked up in the assessment.
This will allow the individual to build the foundational strength in a non-weight bearing fashion, ultimately laying a solid foundation for the progression to more advanced strength and stability exercises.
Eversion Strengthening with a Resistance Band
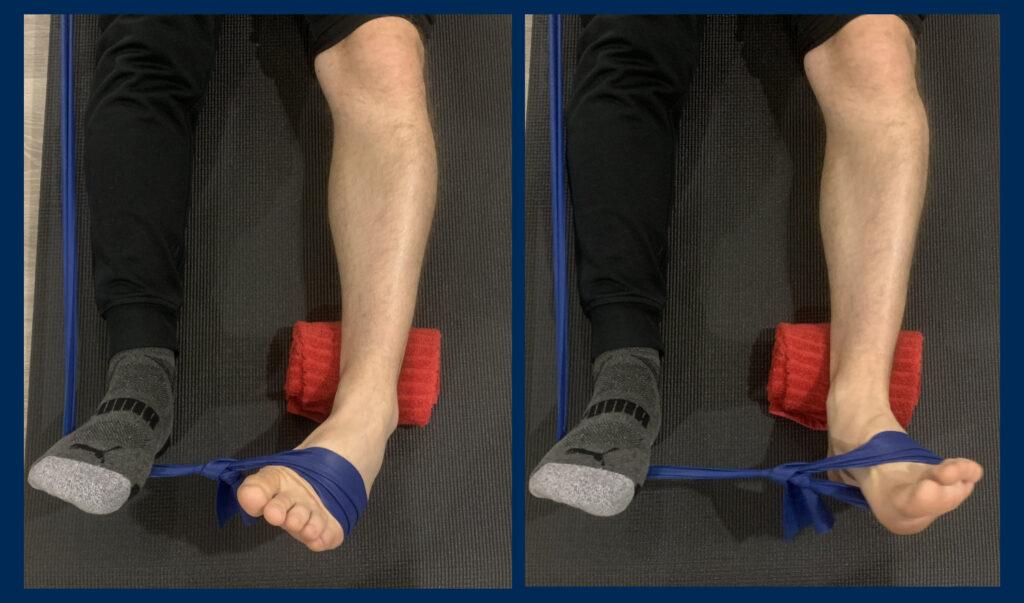
Inversion Strengthening with a Resistance Band

Once the patient is comfortable performing exercises on their feet, physical therapy will quickly move on to dynamic functional strengthening (e.g. various forms of squats) and single leg stability.
Over time, as the patient continues to increase their strength and stability on their feet, especially when they’re on the affected foot only, then we can begin improving stability in circumstances that more closely resemble situations when they may have previously been injured. This is often regarded as the “return to sport” phase of physical therapy.
This is why it’s imperative to ensure a gradual progression of therapeutic exercise and track the patient’s progress with objective strength/balance/stability measures along the way. These more advanced exercises typically involve movement, whereby they have to react quickly to external forces while maintaining proper coordination of multiple segments.
Finally, jumping and return to sport is the cherry on top. The reason this is important is because these activities mimic situations where the person may particularly want to avoid injury, and they may also be motivated to return to these activities with confidence if their ankle is limiting their participation.
Again, it is imperative that the physiotherapist re-assess with objective measures at each visit to ensure proper criteria has been met in order to progress to this phase, especially if jumping is involved, as that represent a high rate of loading that the ankle has to accommodate in a very short amount of time.
How does strength and stability reduce chronic ankle pain?
It’s understandable that this approach to a sprained ankle is counterintuitive to many people, particularly for those seeking a quick fix. While a variety of passive modalities may help in temporary pain reduction (see below), functional strength and stability represent a more long term solution to resolving chronic ankle instability and associated chronic ankle pain from that has occurred from repeated sprains.
What we often see is an initial increase in function with the similar levels of pain, after which symptoms reduce as the ankle joint is more capable of distributing forces away from previously injured areas. This redistribution of forces through the ankle thus allows for continued offloading and healing of affected structures and will offer an effective way to minimize the risk of repeated ankle sprains.
What other things in a physio clinic can help with a chronic ankle sprain?
There are many passive modalities that can be employed as an adjunct to activity-based rehab which can allow for improved comfort throughout the process. Examples include transcutaneous electrical nerve stimulation (TENS), interferential current (IFC), intramuscular stimulation (IMS), dry needling, ice (particularly in cryo-cuff form), heat, low grade joint mobilizations, and soft tissue release.
While these are great adjuncts to treatment that can help with ankle pain, they usually don’t provide a long term solution to addressing chronic ankle sprains, especially if chronic ankle instability has indeed been identified as the main source of problems.
Can an ankle brace help with chronic ankle sprains?
Yes, an ankle brace can help prevent ankle sprains, but should not be relied upon completely for ankle stability.
The best type of ankle brace to help prevent a sprained ankle are lace-up ankle braces, or ankle stabilization orthoses (ASO’s). These use a more firm fabric that helps to prevent excessive inversion and eversion of the ankle joint, and while some people find them a little bulky, they can in fact fit under a shoe.
Summary
Overall, if you’re concerned about a history of ankle sprains that has resulted in nagging pain, a visit to a physiotherapist is highly recommended. While cases vary on an individual basis, be prepared for some physical testing and to incorporate strength and stability exercises into your treatment in order to help resolve chronic ankle instability.
We hope this article helped provide insight into why repeated ankle sprains may result in chronic ankle pain, but when in doubt, asking your physiotherapist to explain their reasoning can provide further clarification, and may even provide more motivation for yourself in the process.
References
Al Adal S, Pourkazemi F, Mackey M, Hiller CE. The Prevalence of Pain in People With Chronic Ankle Instability: A Systematic Review. J Athl Train. 2019 Jun;54(6):662-670. doi: 10.4085/1062-6050-531-17. Epub 2019 Jun 11. PMID: 31184959; PMCID: PMC6602397.
Cuthbert SC, Goodheart GJ Jr. On the reliability and validity of manual muscle testing: a literature review. Chiropr Osteopat. 2007 Mar 6;15:4. doi: 10.1186/1746-1340-15-4. PMID: 17341308; PMCID: PMC1847521.
De Paepe, A., & Malfait, F. (2012). The Ehlers–Danlos syndrome, a disorder with many faces. Clinical genetics, 82(1), 1-11.
Disclaimer:
The content here is designed for information & education purposes only and is not intended for medical advice.













